Retinal Implants: How Tech Restores Sight
Retinal implant: The truth about bionic vision technology
The promise of the retinal implant sounds revolutionary: restore sight when photoreceptors fail. However, reality proves far more nuanced than the headlines suggest. Recently, social media buzzed with claims about devices that could bypass the cornea entirely. For example, a popular Reddit discussion explored a “futuristic eye implant” concept that bypasses the cornea. Consequently, separating genuine progress from wishful thinking becomes crucial.
After covering bionic vision projects across labs and clinics for years, I can state this definitively: modern retinal implant technology works—but within strict limits. These devices help with light perception, object localization, and safer mobility. They remain far from camera-quality replacement vision. Still, for carefully selected candidates, the impact can transform daily life.
Advertisement
What is a retinal implant? Understanding the core technology
A retinal implant functions as a microelectronic array that stimulates surviving retinal neurons. Specifically, it replaces lost photoreceptor input with electrical signals the brain interprets. In simpler terms, it gives your retina a new pathway to communicate with your visual cortex.
Not all retinal implant designs work the same way. Position and approach determine both performance and limitations:
- Epiretinal systems sit on the retina’s inner surface and stimulate ganglion cells directly, typically using video from an external camera. Benefits include surgical accessibility and well-understood stimulation patterns. The wiring can be delicate, and visual percepts often feel coarse.
- Subretinal arrays slide underneath the retina where photoreceptors once functioned and often use photodiodes to convert light into electrical current. This preserves natural eye movements for scanning, but surgical space is tighter and power is constrained.
- Suprachoroidal placement positions the array between the choroid and sclera, offering safer access and gentler retinal handling. The greater distance from target neurons can reduce visual resolution.
- Optogenetic prostheses use gene therapy to make retinal cells light-sensitive and rely on specialized goggles to project amplified light patterns. This avoids permanent hardware on the retina but requires gene delivery and bespoke optics.
Some epiretinal systems have achieved regulatory approval and limited commercial availability, while others remain in clinical trials. Understanding which options are proven today—not just sci‑fi concepts—matters enormously. Hype often outpaces clinical progress; the viral cornea-bypassing idea is a reminder to demand trial data rather than headlines.
How retinal implant surgery works: From procedure to perception
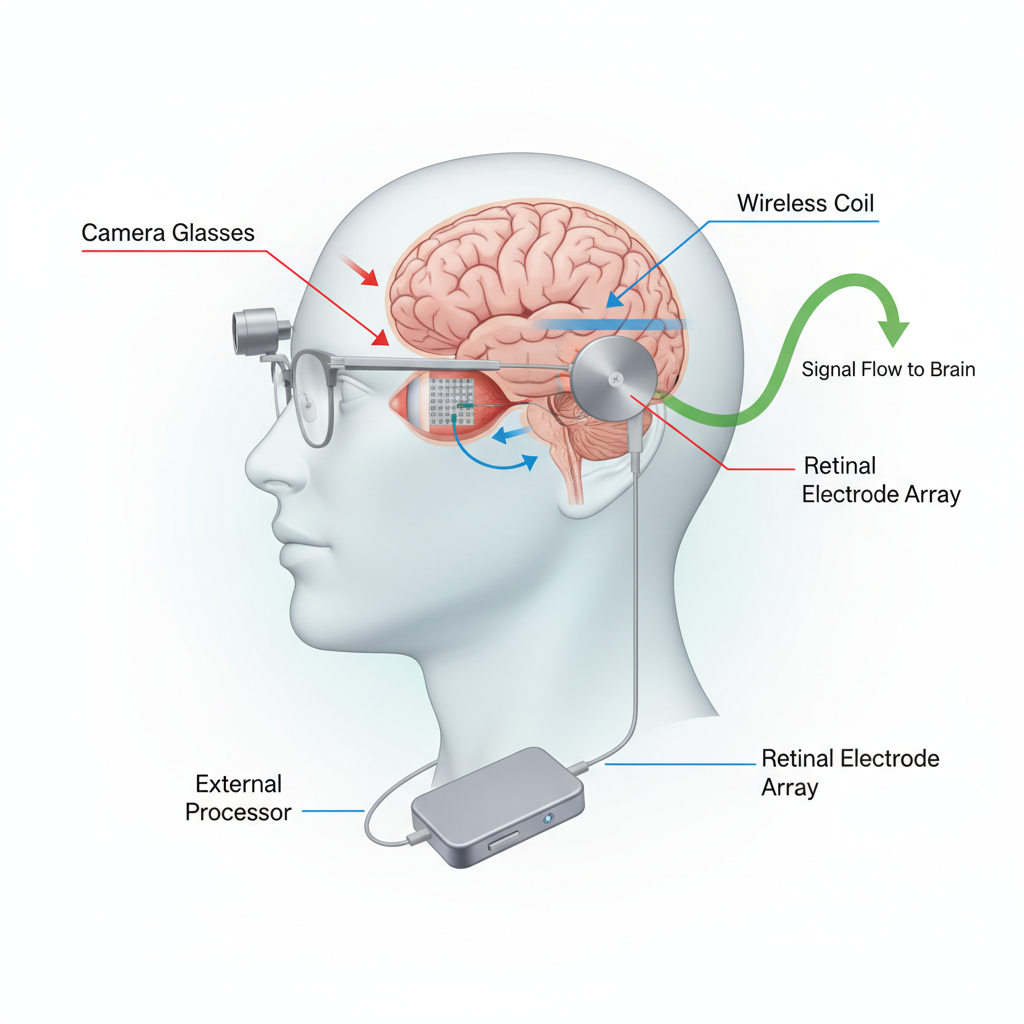
Think of a retinal implant system as a pipeline: capture light, process patterns, deliver current, create perception. Each stage shapes what users ultimately experience.
- External camera and processor: Glasses or head-mounted cameras capture scenes. A pocket processor filters edges, contrast, and motion while shrinking images to match the array’s limited electrode count.
- Implant array: A microelectrode grid sits epi-, sub-, or suprachoroidally. Each electrode activates a cluster of neurons, generating tiny flashes called phosphenes.
- Power and data transmission: Power and data reach the implant through wired leads and wireless coils; optogenetic systems use precisely controlled light instead.
- Retinal interface: Carefully calibrated pulses encourage repeatable phosphenes. Over time, the brain learns to interpret these patterns as edges, doorways, or navigation cues.
Surgery typically involves a vitreoretinal surgeon and general anesthesia. For epiretinal arrays, surgeons secure the array to the retina and route thin cables to receiver coils. Subretinal and suprachoroidal placements use different approaches but share goals of stable placement and reliable connections.
Most patients return home within one to two days, though initial healing takes several weeks. Teams activate the device only after the eye is stable. Expect multiple programming sessions to map phosphenes and calibrate stimulation.
Activation day marks just the beginning. Users work with low-vision therapists to build a visual vocabulary: starting with light detection and target tracking, then progressing to doorways, hallways, and navigation markers. Reset expectations: retinal implants rarely restore face recognition or fluent reading. Typical gains include improved light perception, object detection, and enhanced orientation and mobility. Outcomes vary with diagnosis, remaining retinal health, and training commitment.
Early functional gains may appear within weeks, but meaningful improvements often require months of dedicated practice. The brain is learning an entirely new visual language.
Retinal implant candidates: Who qualifies and what are the risks?
Candidate selection demands careful evaluation and collaboration. The best outcomes occur when disease has destroyed photoreceptors while preserving inner retinal circuitry.
- Common medical indications: Advanced retinitis pigmentosa and other inherited retinal degenerations with minimal remaining central vision.
- Retinal integrity: Clinicians assess whether ganglion and bipolar cells remain present and responsive to electrical stimulation.
- General health: Candidates should tolerate eye surgery and commit to extensive rehabilitation; age matters less than overall health and motivation.
Risks include surgical complications such as infection, retinal detachment, hemorrhage, and inflammation. Device-specific risks include lead breakage, electrode failure, or the need for revision surgery.
- Resolution limitations: Today’s arrays contain far fewer “pixels” than camera sensors, so expect coarse vision that requires significant training for practical utility.
- Longevity and support concerns: Electronics can fail and companies can change direction; patients should investigate long-term service commitments and upgrade pathways.
- Rehabilitation demands: Success requires substantial training time, particularly early on, and not everyone adapts at the same pace.
Decisions hinge on personal goals. Some patients value independent navigation over detailed vision; others prioritize recognizing high-contrast objects at home. Aligning implant strengths with individual goals is essential.
Alternatives continue to evolve: gene therapies aim to slow degeneration or restore proteins, and stem cell approaches aim to rebuild photoreceptors. These suit different disease stages, so a retina specialist can map optimal paths.
Flashy headlines often distort expectations. Hype centers on dramatic leaps like cornea-bypassing beam systems; compare each claim against clinical trial endpoints and demand data rather than marketing copy. The Reddit thread about a cornea-bypassing retinal concept is a useful reminder to trace claims back to evidence.
Preparing for retinal implant surgery and long-term success
Preparation resembles training for a marathon rather than a sprint. Comprehensive planning sets the foundation for optimal outcomes.
- Specialist evaluations: Meet retina surgeons, low-vision optometrists, and rehabilitation teams. Expect visual field testing, OCT scans, and sometimes ERG assessments.
- Imaging and surgical planning: High-resolution scans guide array placement and assess retinal health; anatomy influences whether epi-, sub-, or suprachoroidal placement is best.
- Counseling and goal-setting: Establish concrete targets like spotting door frames or following sidewalk edges; realistic goals outperform vague hopes.
After surgery, rehabilitation drives progress. Activation begins with mapping phosphenes and identifying comfortable stimulation settings. Early sessions often feel abstract, but patterns become meaningful over time.
- Vision training: Exercises build scanning techniques, head movement strategies, and contrast utilization skills so users can “read” edges and motion cues.
- Orientation and mobility: Specialists can integrate white canes or guide dogs as needed; the implant adds a new information layer for safer travel.
- Device tuning: Firmware updates and algorithm adjustments can sharpen contrast and reduce noise; expect periodic recalibration sessions.
Timelines vary: some patients report useful gains within a month, others need several months of consistent practice. Consistency and home support are vital.
Long-term life with a retinal implant includes ongoing maintenance and community. Keep routine follow-ups to monitor eye health and hardware, and ask about upgrade paths for cameras, processors, and software improvements.
- Device care: Protect external components from moisture and impact; learn basic troubleshooting for coils, cables, and chargers.
- Clinical trial opportunities: Trials may offer access to newer arrays, smarter algorithms, and hybrid approaches—ask your team about eligibility and transfer pathways.
- Support networks: Peer groups share training tips, daily strategies, and motivation; real user stories beat marketing copy.
Maintain balanced expectations: a retinal implant is a powerful tool, not a cure. When used effectively and paired with dedicated training and patience, it can amplify the visual information your brain receives and reopen parts of the world you’ve missed.
If headlines about beaming images to the retina sparked your curiosity, dig deeper: ask specialists challenging questions and insist on data from controlled trials. Public debate is useful, but real progress happens in clinics and training rooms where patients transform electrical pulses into meaningful perception.
The bottom line: for carefully selected individuals, a retinal implant can significantly boost independence and confidence. It won’t fully restore natural vision, but it can restore life-changing options—progress worth supporting.
For more on AI & Technology, check out our other stories.


Leave a Reply